





















The Child Opportunity Index (COI) was developed in 2014 to measure and map "the quality of resources and conditions that matter for children to develop in a healthy way" in the neighbourhoods they grow up, and to spark conversations about inequality and encourage actions to increase equity. In 2020, COI 2.0 was launched including updated data (via) from 29 neighbourhood-level indicators covering three domains: education (quality and access to early childhood education, social resources related to educational achievement), health and environment (access to healthy food and green space, pollution from industry, exposure to extreme heat), social and economic domain.
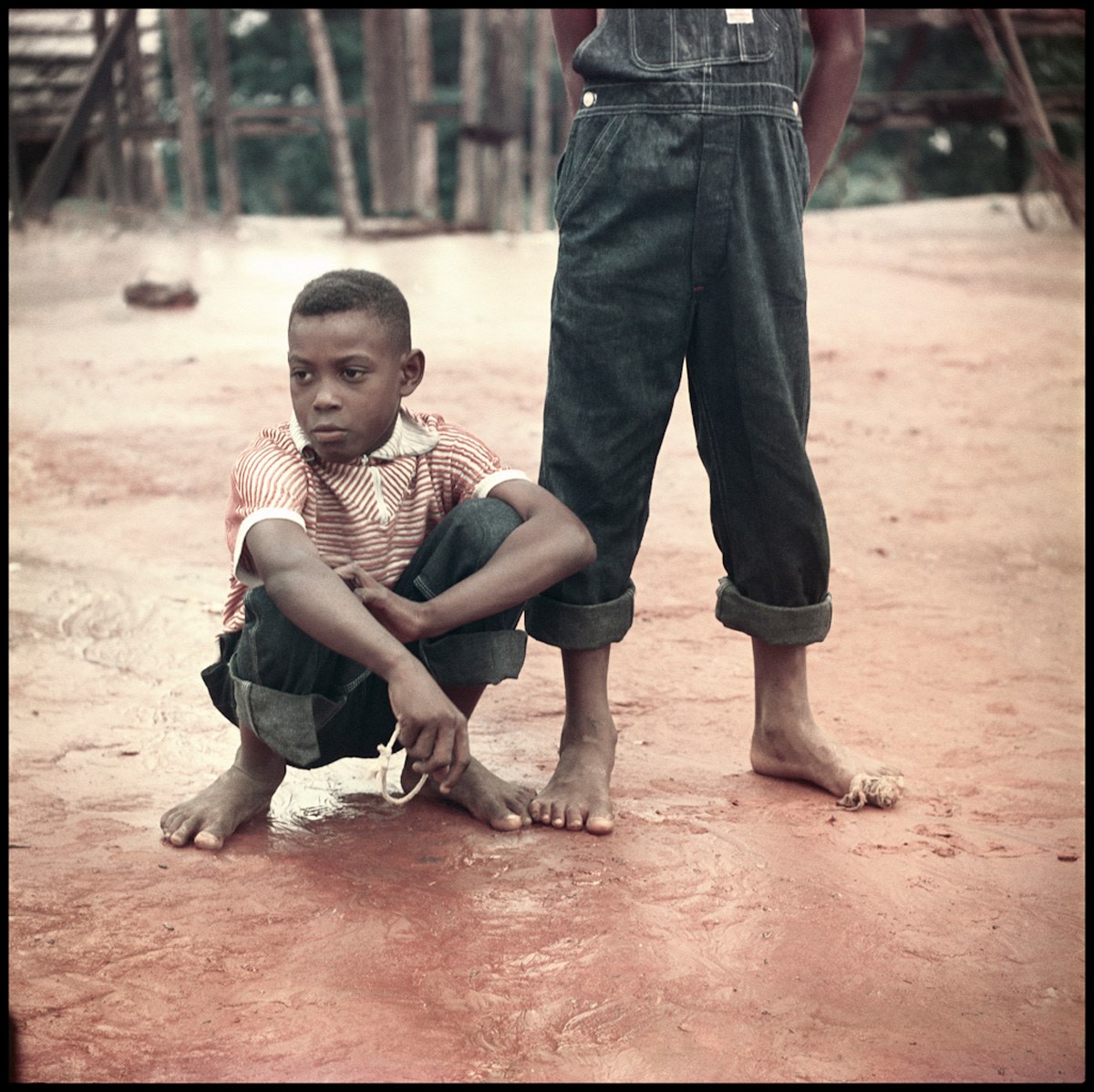
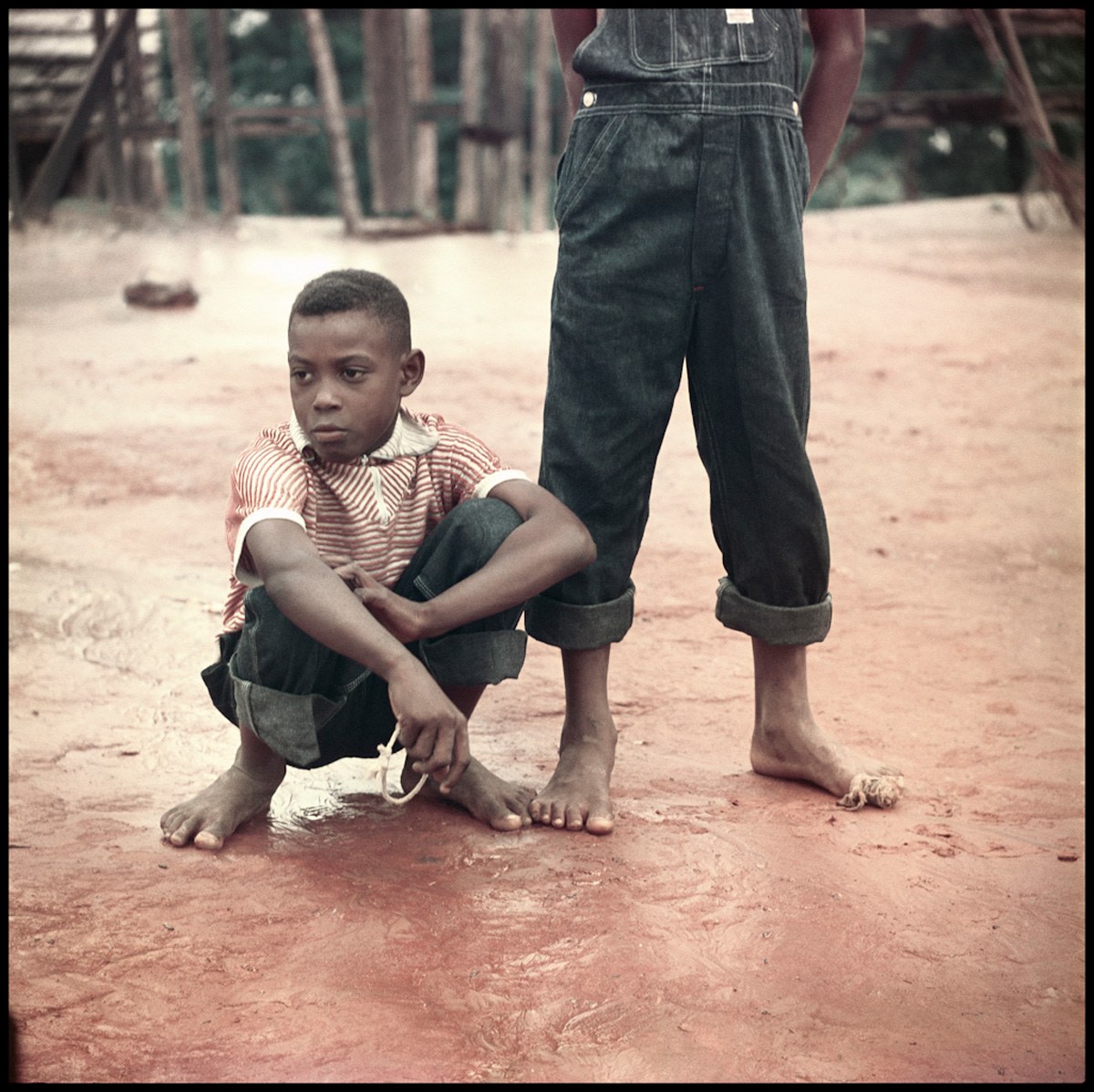
Good schools, parks, playgrounds, healthy food, clean air, safe housing, health care are some aspects crucial for children to become healthy adults. In the United States, many children live in these "high opportunity" neighbourhoods that provide access to the conditions mentioned before. Many, however, live in "low opportunity" neighbourhoods, many of these "many" being Black, Hispanic and Native American children (via).
For example, (...) in the Milwaukee metro the typical White child enjoys a neighborhood with a Child Opportunity Score of 85, while the typical Black child lives in a neighborhood with a score of only 6. As another point of comparison, this racial gap in Milwaukee represents about four opportunity levels (the maximum possible): the typical Black child lives in a very low-opportunity neighborhood, while the typical White child lives in a very high-opportunity neighborhood. (via)

As of 2017...
While only 9 percent of white children live in the 20 percent of neighborhoods ranked as lowest in opportunity, 32 percent of Hispanic and 40 percent of black children live in such neighborhoods. These disparities remain after controlling for children’s own poverty status. Looking just at poor children, 22 percent of white children live in the 20 percent of neighborhoods ranked as lowest in opportunity, but 45 percent of Hispanic and 57 percent of black children live in such neighborhoods (...). As in our analysis of neighborhoods by poverty status, we find that racial/ethnic inequities in neighborhood opportunities for children are larger in metro areas with higher levels of segregation. (McArdle & Acevedo-Garcia, 2017:5)
Summing up...
Segregation is not benign. The neighborhoods where children live and grow are both separate and greatly unequal along racial/ethnic lines in ways that have profound impacts on opportunities for healthy child development and wellbeing. The differences in neighborhood characteristics and opportunities between racial/ethnic groups are dramatic not just on average, but for large majorities of their populations. (McArdle & Acevedo-Garcia, 2017:4)
- - - - - - - - - - - - - - -
- McArdle, N. & Acevedo-Garcia, D. (2017). Consequences of Segregation for Children's Opportunity and Wellbeing; via
- photograph by Gordon Parks (Alabama, 1956) via and via





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}